

Early this year we were alerted to the plight of a 14-year old Kokoda schoolgirl who needed a a lifesaving heart operation – one that had to be performed overseas due to the medical complexity of her condition.
‘Our daughter’s health is our priority and the further delay of her operation has been a concern for us which is becoming desperate, thereby resulting in our plea for your assistance’ wrote Mrs Doreen Dumu, a nurse at the Kokoda Hospital on 29 January 2019.
Her daughter, Freda, has a ‘tetralogy Fallot‘ which is a serious congenital heart defect. The surgery she requires is not available in PNG and the cost of the operation and rehabilitation in Australia was in excess of $100,000.
We contacted the PNG Kokoda Track Authority (KTA) and suggested that they get every trek operator to submit the name and contact details of each of the trekkers they would be leading across the trail during the Anzac period – a practice that should have been put in place a decade ago to capture the contact details of the 50,000 Australians who have trekked Kokoda since then. Unfortunately numerous requests to establish such a database for fundraising purposes over the years have been ignored.
Their refusal to assist Freda was perplexing in view of an earlier decision by their Acting CEO to ‘donate’ $150,000 to an Australian NGO to hand-out as ‘educational supplements‘ to local villagers on and beyond the Kokoda Trail. Calls for those funds to be reimbursed have been ignored.
We also sought assistance from a close friend and supporter, Jeff Hudson, a Director of the Children’s First Foundation. Jeff worked tirelessly to help ‘create the miracle‘ for Freda but as it transpired it was beyond their resources.
We then tried Rotary Oceana Medical Aid for Children (ROMAC). They were also keen to assist but there seemed to be an issue with Children’s Hospitals in NSW accepting patients from the Pacific.
We wrote to the Minister for Health to see if he could check it out on our behalf but didn’t receive a response.
We also arranged for Emily Kleing from the Oro Community Development Project to assist us with any liaison necessary as she is now residing in Port Moresby, We had previously worked with Emily to help build a TB Isolation Ward at the Popondetta Hospital,
We then published a Facebook post to ‘help reverse the death sentence for a 14 year-old Kokoda schoolgirl’ and invited trekkers to contact the KTA to support our fundraising efforts but they continued to ignore her plight.
Just as we neared the edge of desperation an ‘Angel’ emerged from PNG:
Dear Charlie,
I am so very pleased to inform you that Pastor Dr Kirk head of our Paediatric cardiology partners “ For Hearts and Souls” will be organizing free surgery for Freda in San Antonio, Texas USA.!!
Dr Kirk and team have successfully provided minimal invasive approach to repairing congenital heart defect for 13 PNG children at our PIH cath lab and arranged treatment for 2 very complicated children at the Mayo clinic in the US.
Freda‘s family prayers ensured that I read your post on FB ( I don’t do FB regularly anymore) and was able to contact Dr Kirk before he and his team left Moresby this afternoon, upon completion of their second mission at PIH.
We will contact the patient and you once we receive more information from US.
I trust the Kokoda track foundation will be able support the travel expenses for the girl and a guardian.
FB has received bad press recently for invasion if privacy and manipulations etc but I am glad it connected us to help this girl and hopefully save her life!
God bless
Dr Amyna
We responded immediately and agreed to underwrite any flight and accommodation costs for Freda and her guardian – I contacted the Chairman of Network Kokoda, Andrew Tracy, who agreed to support any necessary fundraising endeavours.
As it transpired I had met Dr Amyna Sultan 10 years ago but had never seen her!
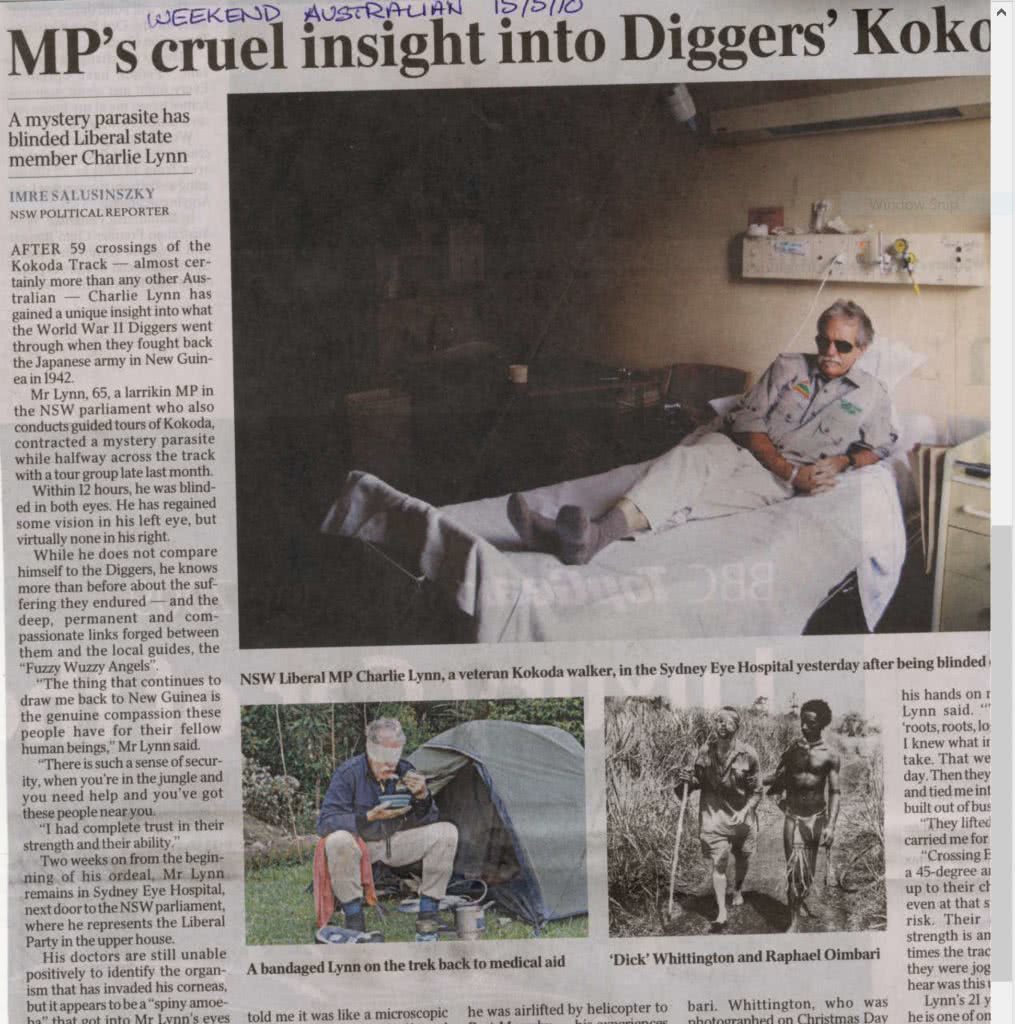
I had been evacuated from the trail by helicopter after losing my sight half-way through a trek. It was a Saturday afternoon and she was off-duty but responded to an urgent call for help from the duty nurse at the Pacific International Hospital – If she hadn’t I would be blind today. It was still a close call however and eventually took five weeks of intense specialist treatment at the Sydney Eye Hospital to restore it as best they could. You never forget things like that!
Dr. Gerard Sutton
Cornea Specialist Sydney Eye Hospital Sydney, NSW
May 1, 2009Dear Dr. Sutton,
Re: Urgent Referral for Mr. Charlie Lynn, DOB 14-1-1945I am referring Mr. Lynn, a 65 year Australian man who is a member of NSW parliament, and operates a Kokoda trekking expedition in PNG, for further management of presumed acanthamoeba vs bacterial keratitis in both eyes
Mr. Lynn presented to our clinic this morning with a two day history of severe pain, redness and poor vision in both eyes. He is a myope who uses extended wear ( monthly disposable) soft contact lenses when he comes up to Kokoda for the expeditions four times a year, for many years now and gives a history of bathing in the river without removing his contact lenses!
He reported that he developed severe pain in both eyes 2 days prior to presentation following his evening wash in the river. He had come into close contact with a local person with presumed “red eyes” the samaday_Unfortunately, he did not remove his contact lenses which he had been wearing for past 5 days, for another 24 hours until his symptorrs got worse.He then removed the contact lenses and the eyes were patched with antibiotic eye ointment for a whole day before we saw him. He was started on Flucloxacillin and Nurofen by a doctor on the expedition.
His past ocular history is significant for excision of a left lower lid benign skin lesion . There is no history of “cold sores” or any eye infection or inflammation. He is otherwise in good health and has no known drug allergies.
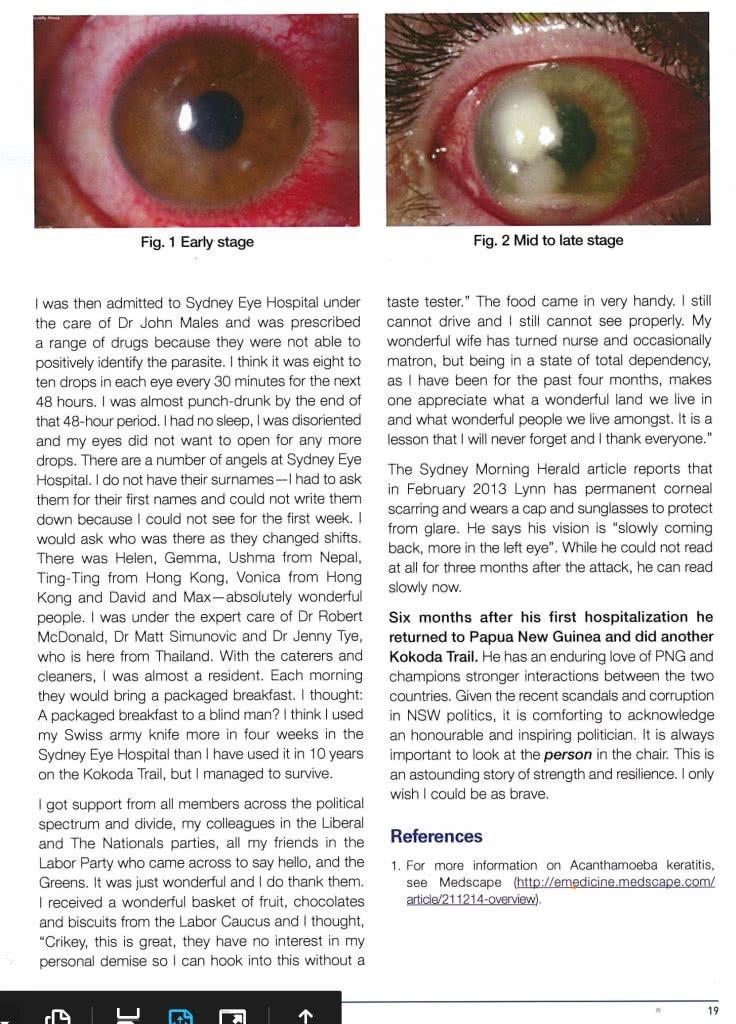
On examination, his visual acuity was hand movement in the RE and counting fingers at½ m in the LE. He was in pain and was extremely photophobic. Pupils were normal. There was diffuse conjunctiva! hyperemia in both eyes. The corneas in both eyes were 80% denuded of their epithelium with large central epithelial defects about 8 mm in size. Corneal stroma was clear and compact. There were no infiltrates in the stroma in both eyes. The endothelium was coated with inflammatory exudates from hypopyon (20%) in the anterior chambers of both eyes. The anterior chamber was deep and the pupil was round. There was 2 + nuclear sclerosis in both lenses.
My clinical working diagnosis was of bilateral acanthmoeba keratitis or some form of severe epithelial bacterial keratitis. I did scrape some of the remaining corneal epithelium from both eyes which was sloughing off to make slides and culture the plates. The Giemsa and gram stain slides revealed plenty neutrophils and some lymphocytes but no organisms were seen. KOH prep was negative. I will inform you of any positive culture growths when the plates are read by our laboratory.
Meanwhile, I have started the patient on Brolene drops 0.1% q 30 mins during the day and q hourly during the night, Norfloxacin eye drops and Torbamycin eys drops q alternate hour in both eyes round the clock and Cyclopentolate 1 % tid. I have also started Ketoconazole 200 mg qd, as we do not have Voriconazole or ltraconazole available here in Moresby. He will be returning back to Sydney on tomorrow (Sunday) afternoon’s flight and has been advised to go straight to the emergency at SHE.
I believe you have a confocal microscope and PCR facility at you institution which may aid in more definitive diagnosis and proper treatment to salvage these eyes.
Thank you for accepting the patient and I look forward to receiving a follow-up on Mr. Lynn.
Regards
Dr. Amyna Sultan Diplomate ABO, (USA) Consultant Ophthalmologist amynasultan@yahoo.com
P.0. Box 6103, Boroko, NCO, Papua New Guinea Ph: 323-4400 I Fax: 323-4600 (Hospital)email: pih@daltron.com.pg

I later learned that Dr Amyna Sultan OBE is a Director and Consultant Ophthalmologist at the Pacific International Hospital in Port Moresby. She is not only a highly qualified specialist but is renowned for her philanthropic work throughout PNG.

Just as we were getting concerned about the time it was taking to arrange for Freda’s operation in Texas, USA our ‘Angel’ made another appearance late yesterday:
Dear Charlie,
We finally have good news for Freda!
We have received a sponsor’s letter to apply for a US visa.
Surgery is planned for late January.
Thanks for your support.
Regards and Happy holidays!
Dr Amyna
Christmas doesn’t get any better than that for Freda, her parents, Doreen and Panuel – and for us! I’m now looking forward to catching up with Dr Amyna when I’m next in Port Moresby so that I can finally get to see her and thank her once again.
Link to Interview with the Sydney Morning Herald over lunch at the Sydney Eye Hospital:






{kind=link}